
{kind=link}

The government body that recommends whether to bring sick refugees from Nauru and Manus Island to Australia for medical treatment was designed to consider not just the advice of doctors, but also the cost and legal implications of the transfers, a document obtained by BuzzFeed News reveals.
Government officials have previously publicly insisted that the medical status of the refugees was the only consideration guiding the decisions.
A draft minute establishing the powerful and secretive Transitory Persons Committee (previously the Transitory Persons Complex Case Review Committee), obtained by BuzzFeed News through freedom of information processes, indicates that the body’s founding purpose was to take into account a much broader array of considerations than refugees’ best medical interests. The committee consists of senior members of the Department of Home Affairs.
The committee’s purpose is to consider the “medical, legal, diplomatic, policy and financial implications” of medical transfers to Australia, according to the draft minute sent by then deputy commissioner of Australian Border Force, Cindy Briscoe, to then Border Force commissioner Roman Quaedvlieg in May 2016.
The minute does not say that recommendations should be made only, or primarily, on the basis of medical advice.
Quaedvlieg told BuzzFeed News he recommended the committee be established and gave advice on how it should be set up, but did not see the final minute. "In my public service experience I'd assess that the minute wouldn't have changed substantively in its final form," he said.
The draft minute identified two key issues giving rise to the need for the committee, neither of which directly concerned the quality of healthcare provided to refugees.
The first was that although the government had worked to reduce the number of transfers to Australia, the cases they continued to see were “unique and complex” and there was a “high likelihood that they will become the subject of legal proceedings”.
Another issue identified in the draft minute was that patients were increasingly refusing treatment in detention, which they believed could lead them to be transferred to Australia for medical attention.
The document asserts that, because of these issues, medical transfers required a “stronger governance process” than was in place, “which ensures all elements are considered and documented as the basis for advice to the decision maker”.

The broad range of considerations the committee was to factor in is at odds with the few public statements the government has made about the body.
Appearing before Senate Estimates in October 2017, then assistant commissioner, detention & offshore operations command, Kingsley Woodford-Smith, said that he had the final call on medical transfers, which he made after receiving recommendations from the Transitory Persons Committee.
Woodford-Smith told the Senate he made those decisions on the basis of medical advice. Asked whether he made decisions on the basis only of medical advice, Woodford-Smith said: “That’s correct”.
In December 2018, a spokesperson for the Department of Home Affairs told BuzzFeed News that the committee considered the person's health condition and other factors related to their health and medical treatment.
In response to several detailed questions, a spokesperson for the Department of Home Affairs told BuzzFeed News today that "medical transfers occur on a case-by-case basis, on the advice of treating doctors in PNG and Nauru and in consultation with a medical officer of the Commonwealth."
BuzzFeed News has previously reported that the committee considered the political and legal ramifications of decisions to grant or refuse a transfer request.
For example, in June 2018, the committee heard it was preferable to avoid “close scrutiny” of a case where a refugee had refused a transfer to Taiwan, and which might go to court. In relation to the same case, the committee discussed considering the “reputational risk to the department” and the “precedents” the case would set.
The draft minute setting up the committee also outlined a significant drop in medical transfers from Nauru and Manus to Australia.
In the 2014/15 financial year, 540 people were transferred, including 410 from Nauru. In the 2015/16 year to April 26, 2016 the total number was down by 92.2% to 42.
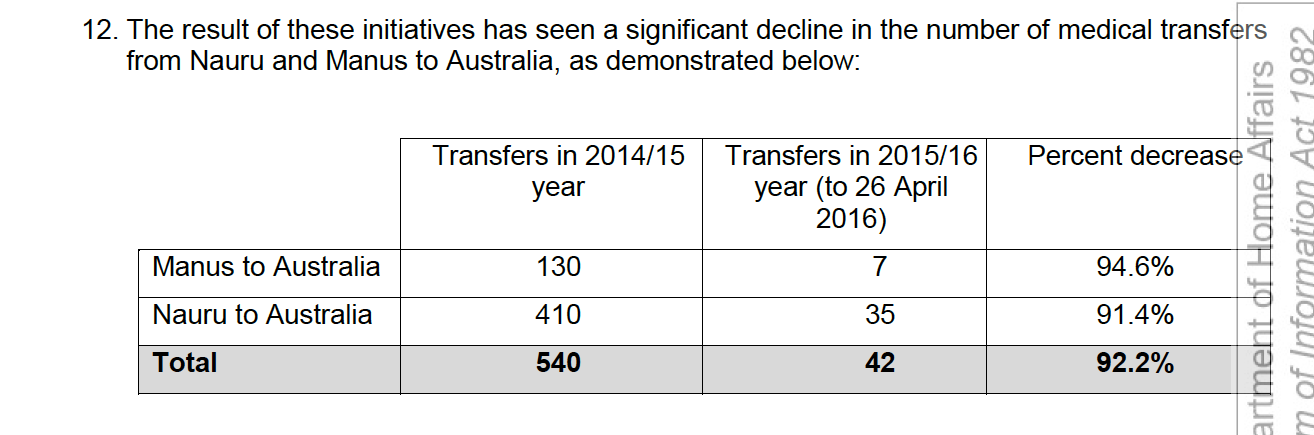
The document attributed the significant drop to a policy change which meant family members were no longer automatically transferred to Australia with a patient, and to the addition of extra medical equipment and doctors to Nauru.
Quaedvlieg said he recommended to departmental secretary Mike Pezzullo that the committee be established, having observed the transfer cases being managed across the department and the ABF “in a disjointed manner”. In May 2016, he came to the view that the coordination of these cases could be improved if a committee was established “which could discuss and assess all of the relevant factors in a case simultaneously”.
“While individual cases were determined primarily on medical advice, any such transfer involved a range of other factors, including legal, diplomatic, policy and logistical considerations, all of which required coordinated input from a range of functions and individuals,” Quaedvlieg said.

A medical transfer panel is not new. One was established in 2016 but became a bureaucratic quagmire. A slimline 5-member panel may work more quickly & AMA representation brings independence, but ministerial override, DHA oversight & ABF secrecy provisions will hobble it I suspect
Quaedvlieg said he provided guidance and advice on how the committee should be “comprised and conducted”, with ultimate responsibility sitting with Pezzullo.
The committee was originally intended to meet daily, but minutes suggest it went months without convening.
It also had no member with a medical background for more than nine months. In Sept. 2017 the department’s chief medical officer (CMO) Dr John Brayley – a member of the committee – suddenly resigned from his post. From then until July 2018 the CMO position was vacant, and another public servant without medical qualifications acted in the position. While medical officers would attend meetings as advisors, they did not have a decision-making role.
The medical transfer process is currently the subject of fierce debate, with a growing push for decisions to be made by doctors instead of bureaucrats. A proposal by independent MP Kerryn Phelps, due to be debated by the House of Representatives next week, would give doctors the final say, unless the immigration minister raised national security concerns.

In response, the government this week proposed establishing a Medical Transfer Clinical Assurance Panel, chaired by the CMO and a membership of doctors, including a trauma expert. The panel could review the department’s decisions and ask the department to reconsider, but would not have override power.
Briscoe and Woodford-Smith declined to comment, as did the public servant responsible for making final edits to the document.